There's no universal answer, but the decision for a patient considering 'stem cell vs PRP' usually breaks down along four axes: diagnosis, evidence quality, cost, and what the marketing is actually saying.
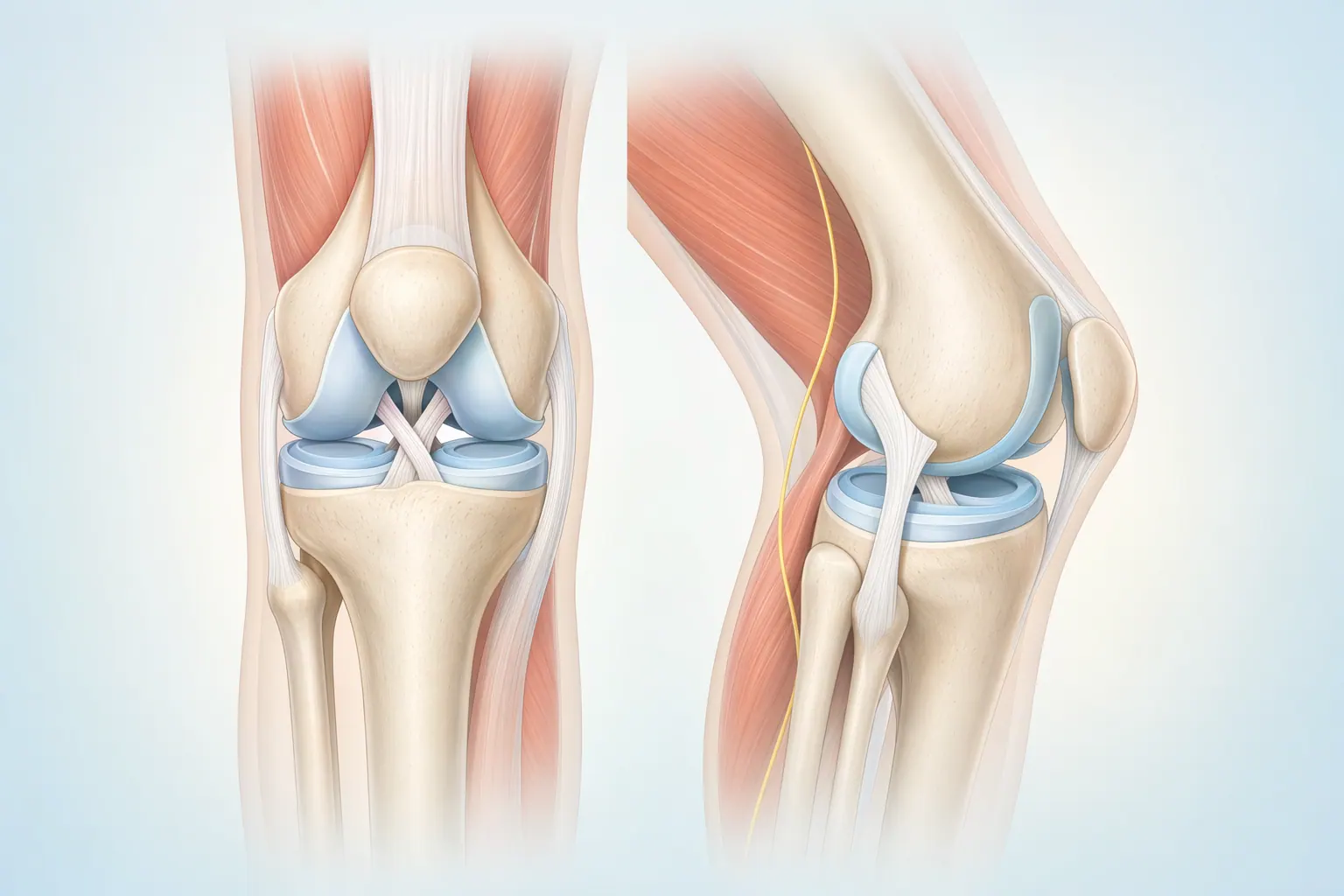
Diagnosis. For most orthopedic problems where biologics help — tennis elbow, patellar tendinopathy, mild-to-moderate knee OA, plantar fasciitis — PRP is the better-supported option. For end-stage joint disease, neither biologic injection meaningfully changes the trajectory. The honest conversation there is about joint replacement, not another injection.
Evidence quality. PRP has 20+ years of published data, with thousands of patients across randomized trials. The evidence is strong for some indications and mixed for others — we'll tell you which camp your diagnosis falls into. 'Stem cell' injections for joint OA have small case series, a handful of small RCTs, and inconsistent preparation methods between clinics. There is no large-scale evidence base supporting routine use.
Cost. PRP is $500–$1,500 per injection. A typical course is 1–3 injections. Stem cell injections at clinics that aggressively market them are $3,000–$8,000 per knee, sometimes more. Neither is covered by insurance. The cost gap is roughly 5x to 10x — for a treatment with substantially weaker evidence.
What the marketing is saying. If a clinic is selling 'stem cells' as a cure for arthritis, promising to 'regrow cartilage,' or pushing a same-day cash-pay decision, that's a real warning sign. The FDA has issued multiple warning letters to clinics making exactly those claims. Honest framing sounds like: 'This is investigational, this is what the published evidence does and doesn't show, and here's why it costs what it costs.' If you don't hear that, slow down.