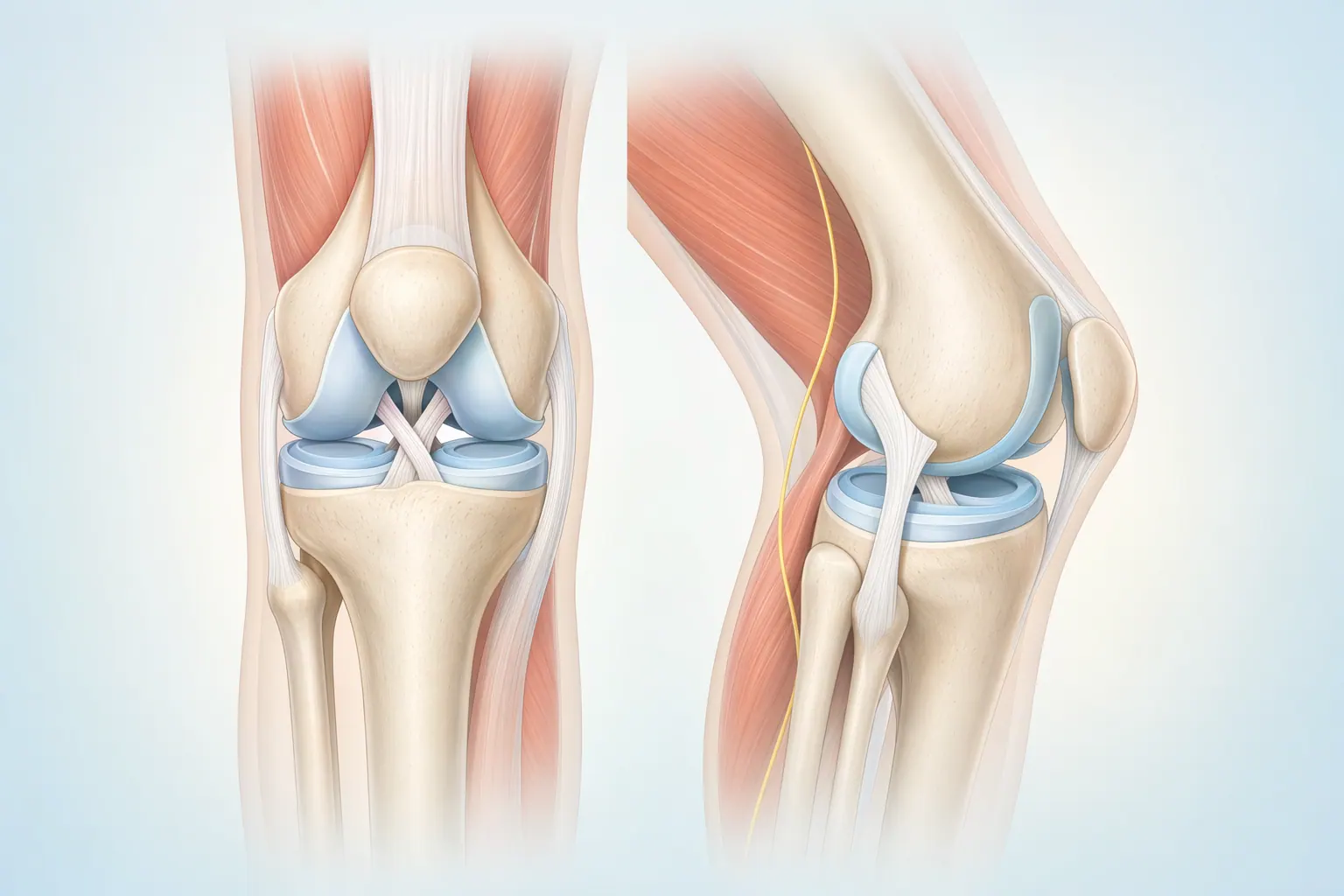
The anterior cruciate ligament — the ACL — is one of four ligaments that hold your knee together. It runs diagonally through the middle of the joint, connecting the femur to the tibia, and its job is to keep the knee from sliding forward and rotating out of place when you pivot, plant, or land from a jump.
Most ACL tears happen in a split second. A soccer player plants a foot and twists. A skier catches an edge. A basketball player lands awkwardly from a rebound. There's often a popping sound or sensation, followed by swelling within a few hours and a knee that suddenly feels unreliable — like it can't be trusted on stairs, slopes, or quick changes of direction.
The injury falls on a spectrum. Partial tears leave some of the ligament intact and may stabilize with rehab. Complete tears — the more common scenario — don't heal on their own, because the ACL lives in a fluid-filled joint that prevents the kind of clotting that heals other ligaments. Whether a complete tear needs surgery is a separate question, and it depends entirely on what you want to do with the knee.
At LAOSS, our sports-medicine surgeons treat ACL injuries every week. We don't push surgery on patients who don't need it, and we don't undertreat athletes who do. The conversation starts with an exam, an MRI when warranted, and an honest look at your goals.