What patients ask us most
- Which one actually works better for knee arthritis?
- Why isn't PRP covered by my insurance?
- How fast does each one work — and how long does it last?
- Can I do both, and in what order?
- Will PRP help me avoid knee replacement?
Both injections are common, both work — but for different reasons, on different timelines, at very different prices. Here's how LAOSS specialists decide which one fits your knee, tendon, or joint, and when it makes sense to use both.

Cortisone calms inflammation. PRP signals healing.
On the surface, PRP and cortisone injections look identical — both are in-office shots, both go into the joint or tendon, both are part of a conservative orthopedic plan. But they do completely different things to the tissue.
Corticosteroid (cortisone) injections deliver a potent anti-inflammatory steroid (typically triamcinolone or methylprednisolone) mixed with a local anesthetic. The mechanism is well-understood — the steroid suppresses the inflammatory cascade that's driving your pain. Relief typically starts within 24–48 hours, peaks at 2–4 weeks, and lasts somewhere between 4 weeks and 6 months depending on the joint and the underlying problem.
Platelet-rich plasma (PRP) injections use the growth factors from your own blood to trigger tissue repair. A small blood draw is spun in a centrifuge to concentrate platelets, which release signals that recruit healing cells to the injured tendon or joint. You don't feel better for 2–6 weeks — and peak benefit often lands at 3–6 months. The goal isn't to silence inflammation; it's to help the tissue actually remodel.
At LAOSS we use both. The question we answer at every visit isn't "PRP or cortisone" in the abstract — it's which one (or both, in sequence) fits your diagnosis, your timeline, your budget, and your activity goals.
Whether it's cortisone to calm inflammation or PRP to stimulate healing, image-guided joint injections are a cornerstone of non-surgical orthopedic care. This short video walks through what to expect.
Animations licensed from ViewMedica · Swarm Interactive
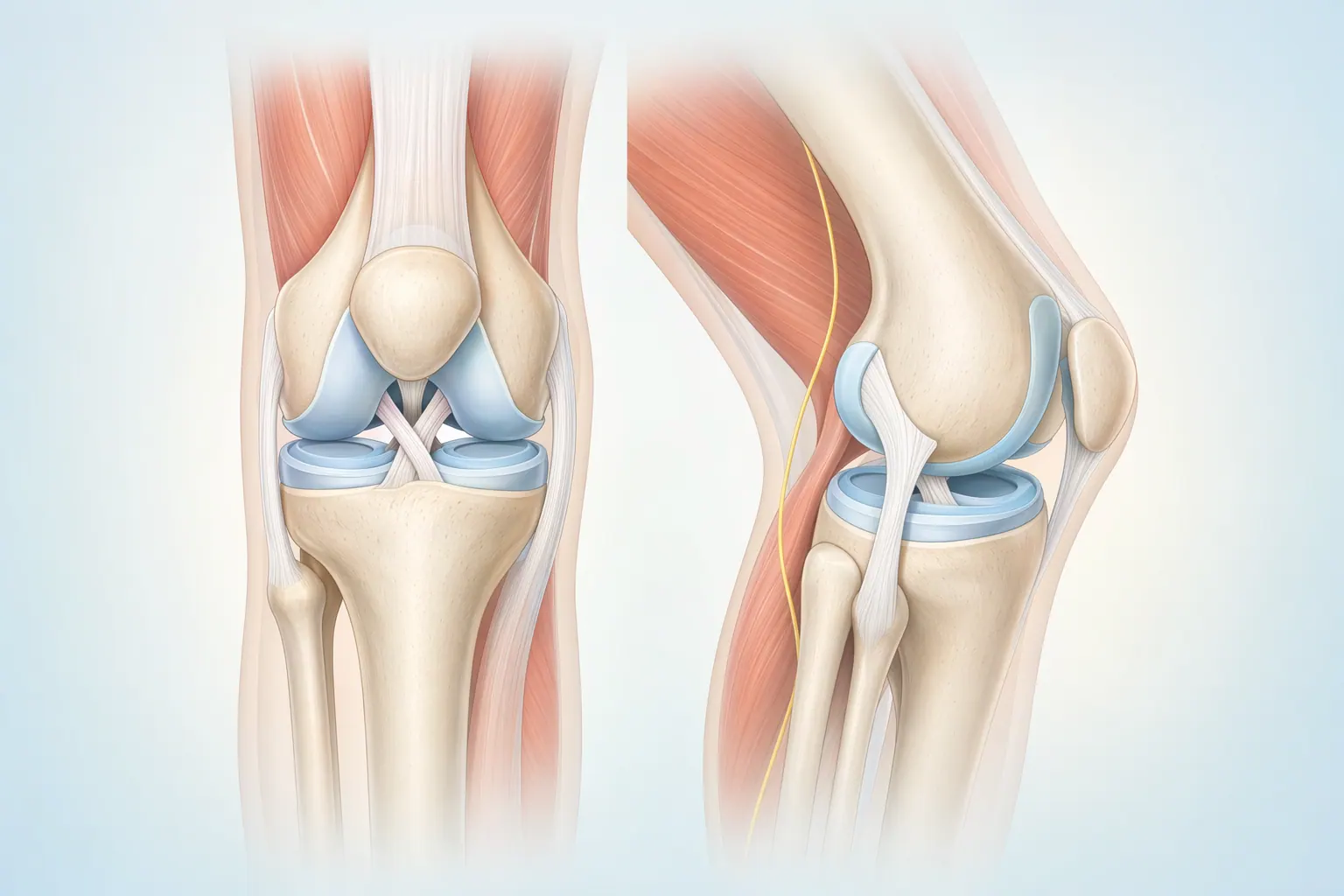
In an arthritic knee, the cartilage is worn, the synovium (joint lining) is inflamed, and inflammatory cytokines flood the joint — that's most of what you feel as pain. Cortisone shuts that inflammatory signal off; you feel better, fast, but the underlying cartilage and tendon damage isn't directly addressed. PRP delivers concentrated growth factors that recruit healing cells to the damaged tissue — slower, but aimed at repair, not just symptom suppression. Two different leverage points on the same problem.
There's no universal answer — but the decision usually breaks down along four axes: diagnosis, timeline, cost, and what comes next.
Diagnosis. Cortisone is a strong tool for inflammatory or arthritic pain — synovitis, knee OA flares, bursitis, impingement. It is a poor (and sometimes harmful) tool for tendon problems, because repeated steroid exposure weakens tendon tissue. For tendinopathy — tennis elbow, patellar tendon, Achilles, plantar fascia — PRP is almost always the better long-term call.
Timeline. Cortisone works fast (24–48 hours), peaks at a few weeks, and fades by 2–3 months in most patients. PRP doesn't really kick in until week 4–6, peaks at 3–6 months, and the benefit can last a year or more for the patients who respond.
Cost. Cortisone is covered by virtually every insurance plan — expect a $30–$100 copay. PRP is usually not covered. Out-of-pocket runs $500–$2,000 per injection depending on the site and whether ultrasound guidance is used, and most courses are 1–3 injections.
What comes next. If you're heading toward a knee replacement, you need to stop cortisone at least 3 months before surgery (it raises infection risk) — and PRP isn't going to change the surgical math. If you're trying to stay out of the OR for another 1–3 years, PRP is the more strategic move.
Most patients don't have to pick one and never touch the other. Here's how we sequence them based on which path fits your situation.
When pain is acute, function is collapsing, or cost is a hard constraint — cortisone moves first.
When tissue healing matters more than fast symptom suppression — PRP moves first.
Cost is often the deciding factor — and unlike a lot of clinics, we quote the number before you commit.
Cortisone injection is a covered orthopedic service under virtually every commercial plan and Medicare. Your cost is typically just the copay for a specialist visit and a small injection fee.
Most insurance plans classify PRP as investigational for orthopedic indications. We tell you the exact number before you book — no surprise billing.
Onset and duration are where these two diverge the most. Knowing the curve helps you plan around real life.
The local anesthetic in the mix gives you a few hours of immediate relief. The steroid kicks in over 24–48 hours and runs its course over weeks to a few months.
PRP works on tissue biology, not pharmacology. The timeline is measured in weeks of remodeling, not hours of pain relief.
We won't oversell PRP, and we won't dismiss cortisone. Here's the honest read on the orthopedic literature, by condition.
Decades of trials support cortisone for short-term pain relief in inflammatory and arthritic joint conditions. The catch is durability and tissue effects with repeat use.
PRP isn't a blanket good idea — it's a strong tool for specific indications. We tell you which camp your diagnosis falls into.
These checklists are a starting point — the final call comes at your evaluation, with imaging and exam findings in front of us.
Cortisone is most often the right first move when symptoms are acute, inflammatory, and you need to function quickly.
PRP is the better call when tissue healing matters more than fast symptom suppression — and when steroid would be the wrong physiologic tool.
Recovery timelines diverge sharply — cortisone is measured in hours and days, PRP in weeks and months.
Cortisone is an in-and-out office procedure. Most patients walk out and resume normal activity the same day.
PRP triggers an inflammatory healing response. You'll feel sore for 2–4 days — that's the response working, not a complication.
PT pairs with both injections. With cortisone, PT happens while the steroid is calming inflammation. With PRP, PT is what locks in tissue remodeling.
It's not unusual to use both — just not on the same day and not in the same way.
A common pattern at LAOSS for knee osteoarthritis: cortisone now to break a severe pain cycle, PRP later to address the underlying tissue. The steroid buys you 6–12 weeks of functional relief while you start physical therapy. Then, once the acute flare is calm, PRP can be considered for the longer-term tissue-level work. We typically wait at least 6–12 weeks between a cortisone injection and a PRP injection in the same joint, because residual steroid in the tissue can blunt the PRP healing response.
For tendinopathies, we generally do not stack them. Repeat steroid exposure weakens tendon tissue, so for tennis elbow, patellar tendon, Achilles, and plantar fascia, the long-term move is almost always PRP rather than serial cortisone.
And there are situations where the answer is neither yet — for early arthritis or mild tendinopathy, structured physical therapy, activity modification, and time often outperform either injection. We'll tell you that too.
Both injections are well-tolerated when delivered by experienced specialists under image guidance — but the risk profiles are different.
Cortisone is one of the most-studied orthopedic interventions. Risks are well-characterized and most are short-lived.
Because PRP uses your own blood, allergic reaction is essentially nonexistent. The real risks are small — the bigger consideration is cost and response variability.
Both cortisone and PRP at LAOSS are performed by board-certified pain management physicians with deep training in ultrasound- and fluoroscopy-guided injection technique. PRP uses our in-house centrifuge protocol — the same physician who does your diagnostic ultrasound prepares the sample and performs the injection. No hand-offs to ancillary staff, no marketing-driven "packages." The person diagnosing is the person treating.
Dr. Acosta saved me from spine surgery. I came in convinced I was going to need an operation. He laid out a non-surgical plan that's been working. So thankful.
Book a visit at any of our eight Los Angeles-area offices. We'll examine the joint, image it on-site, and tell you straight whether cortisone, PRP, both, or neither is the right next step.