Common foot & ankle concerns we treat
- Pain that limits walking, standing, or sleep
- Stiffness, swelling, or reduced range of motion
- Sports injuries — acute or overuse
- Arthritis or post-traumatic joint changes
- Conditions other doctors couldn’t resolve
Hammertoe correction is an outpatient surgery that straightens a bent lesser toe and relieves the pain, corns, and shoe trouble it causes. At LAOSS, board-certified foot and ankle specialists across eight Los Angeles offices tailor the procedure to your specific toe — and only recommend it after conservative care has had a fair chance.

Surgical and non-surgical options at LAOSS.
A hammertoe is a toe — most often the second, third, or fourth — that becomes permanently bent at its middle joint (the proximal interphalangeal, or PIP, joint), so the toe buckles upward in the middle and the tip points down. Over time the tendons and joint capsule tighten around that bend, and the raised knuckle rubs against the top of the shoe. That friction leads to painful corns over the joint, calluses under the ball of the foot, and an aching, cramped feeling that roomier shoes alone no longer fix.
Hammertoes usually start out flexible — you can still straighten the toe with your hand — and gradually become rigid, where the joint no longer moves. This distinction matters a great deal, because a flexible toe can often be corrected by rebalancing the tendons, while a rigid toe usually needs the joint itself reshaped or fused. (Hammertoe is also distinct from a mallet toe, which bends at the joint nearest the nail, and a claw toe, which bends at multiple joints — each calls for a slightly different surgical plan.)
Hammertoe correction is reserved for toes that hurt despite good non-surgical care. The goal is not cosmetic — it is to take the pressure off the painful joint, restore a toe that sits flat and comfortable in a shoe, and stop the corns and calluses from coming back.
This surgical procedure is used to correct a hammertoe, a deformity of the toe that causes the toe to become permanently frozen in a bent position. During this procedure, a small piece of bone is removed to shorten the toe and allow it to straighten.
Animations licensed from ViewMedica · Swarm Interactive
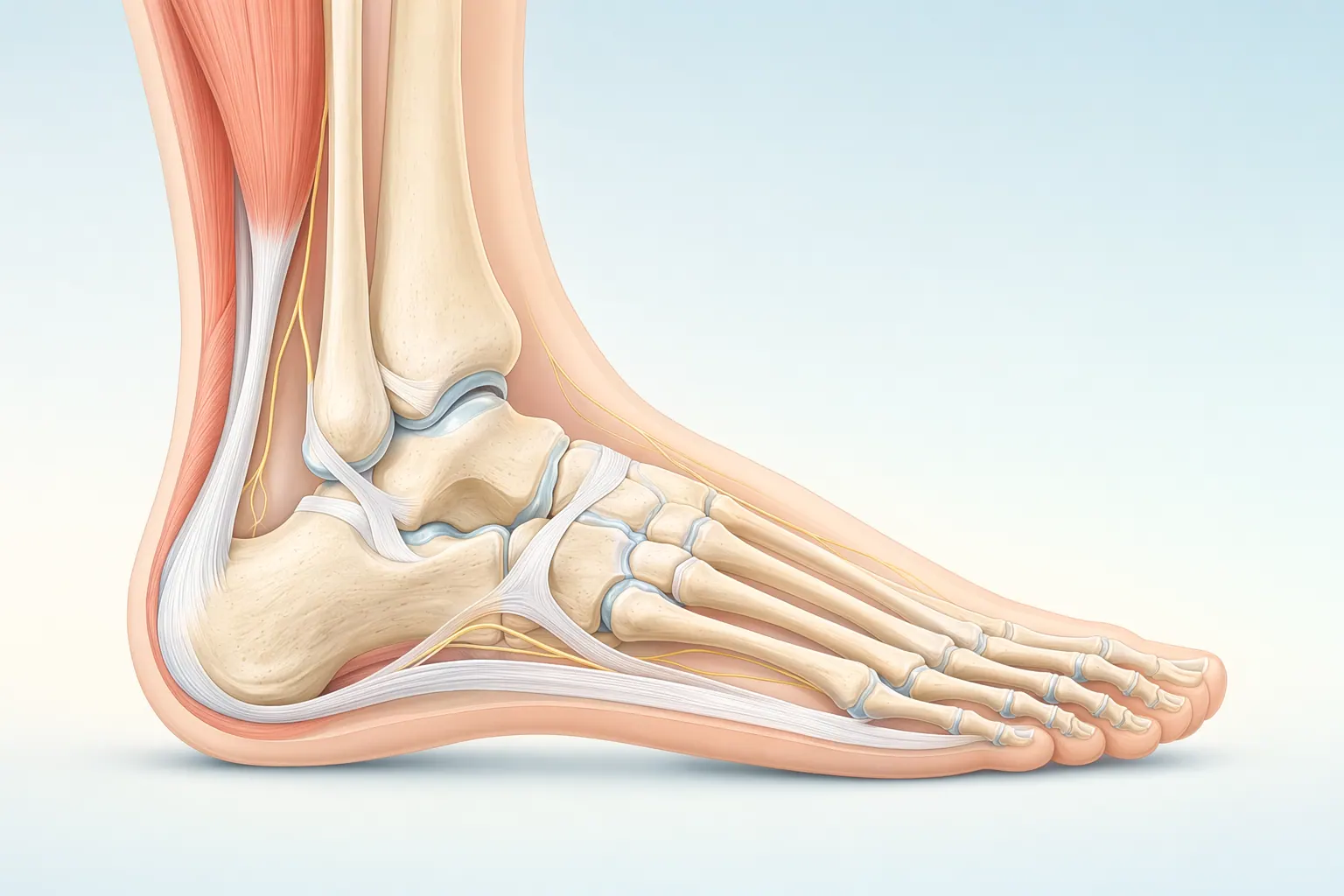
The foot and ankle have 26 bones, more than 30 joints, and over 100 ligaments and tendons. The plantar fascia spans the bottom of the foot, the Achilles tendon anchors the calf to the heel, and the ankle is a hinge that handles every step you take. Most foot and ankle problems trace back to overload, alignment, or footwear that doesn’t match the way your foot is built.
Hammertoe correction is an outpatient procedure, usually done under local anesthesia with sedation or a regional ankle block, and it typically takes 20–45 minutes per toe. Your surgeon chooses the technique based on how flexible the toe still is and which structures are pulling it out of line:
The small incision on top of the toe is closed with sutures, and your foot is dressed and placed in a stiff-soled surgical shoe before you go home the same day.
Foot & Ankle care is highly technique-dependent. Volume, training, and judgment together determine the outcome you actually feel six months later.
Our foot & ankle specialists move stepwise — start with the least-invasive option that fits your situation, escalate only when it doesn't.
If most of these match your situation, an evaluation with a foot & ankle specialist is the next step.
These signs typically point toward an in-person evaluation with a foot & ankle specialist.
Your first visit is built to give you an answer the same day, not just another referral.
Recovery is rarely a straight line — but a clear plan with measurable milestones makes the path predictable.
In the first two weeks we focus on protecting the foot & ankle, calming inflammation, and restoring basic motion.
Targeted physical therapy rebuilds strength, mobility, and confidence in the foot & ankle.
Once function is restored, the focus shifts to keeping you there — and catching any recurrence early.
We talk through the risks and benefits with every patient — informed consent is a conversation, not a form.
Every orthopedic intervention carries a small set of standard risks. We screen, prepare, and monitor for these on every patient.
Some risks are tied to the structures we're treating in the foot & ankle. We discuss these in detail at your visit so you can weigh them against the benefits.
At LAOSS, our foot & ankle specialists combine advanced surgical expertise with a patient-first approach. From minimally invasive arthroscopic techniques to reconstruction, fracture care, and arthritis management, our physicians bring decades of experience to every case. Trusted across Los Angeles, our team is dedicated to restoring mobility, relieving pain, and helping you return to the activities you love.
Most people are pleasantly surprised by how walkable the early recovery is. You will go home the same day in a surgical shoe and can usually bear weight immediately by walking flat-footed, putting pressure through your heel and the back of your foot rather than the toes. We ask you to keep the foot elevated as much as possible for the first one to two weeks — that single habit does more to control pain and swelling than anything else.
If a pin was used to hold the toe, it is typically removed in the office around three to four weeks, which is quick and well tolerated. Stitches come out around the same time. You will transition from the surgical shoe to a roomy, supportive sneaker once the wound is healed and the swelling allows, usually within a month to six weeks.
The honest part: the toe will look and feel swollen and stiff for several months, and mild puffiness can linger longer than you expect — this is normal and improves steadily. Return to driving, desk work, and light activity is often within one to two weeks; standing jobs, longer walks, and exercise come back over the following weeks as comfort allows. We coordinate any needed therapy through your in-network provider and keep a direct line open if anything along the way concerns you.
Book a visit with a foot & ankle specialist at any of our eight Los Angeles–area offices.




