Common foot & ankle concerns we treat
- Pain that limits walking, standing, or sleep
- Stiffness, swelling, or reduced range of motion
- Sports injuries — acute or overuse
- Arthritis or post-traumatic joint changes
- Conditions other doctors couldn’t resolve
Cheilectomy is a joint-preserving operation for hallux rigidus that removes the bone spur jamming the big-toe joint, restoring push-off motion and easing pain. Our foot and ankle specialists offer evaluation and care across eight LA-area offices.

Surgical and non-surgical options at LAOSS.
Hallux rigidus is arthritis of the big-toe joint (the first metatarsophalangeal, or MTP, joint). As cartilage wears down, the body forms a bony ridge or spur on the top of the joint. That spur acts like a doorstop — it physically blocks the toe from bending up, so every step that pushes off the big toe causes a pinching, jamming pain at the top of the joint.
Cheilectomy treats that mechanical block directly. The surgeon removes the dorsal (top-of-joint) bone spur along with roughly the worn upper quarter to third of the metatarsal head. Clearing away the impingement lets the toe dorsiflex (bend upward) again and relieves the pain that comes from bone grinding on bone at push-off. Because the joint itself is preserved rather than fused or replaced, you keep your natural toe motion.
It is important to be honest about what cheilectomy does and does not do. It is a very good operation for the right stage of arthritis — it relieves impingement pain while keeping the joint mobile — but it does not reverse or stop the underlying arthritis. For most patients with mild-to-moderate disease this is the ideal trade-off. For end-stage arthritis, where pain occurs through the entire range of motion rather than just at the end of the bend, a fusion (arthrodesis) is usually the more durable choice, and your specialist will tell you honestly which category you fall into.
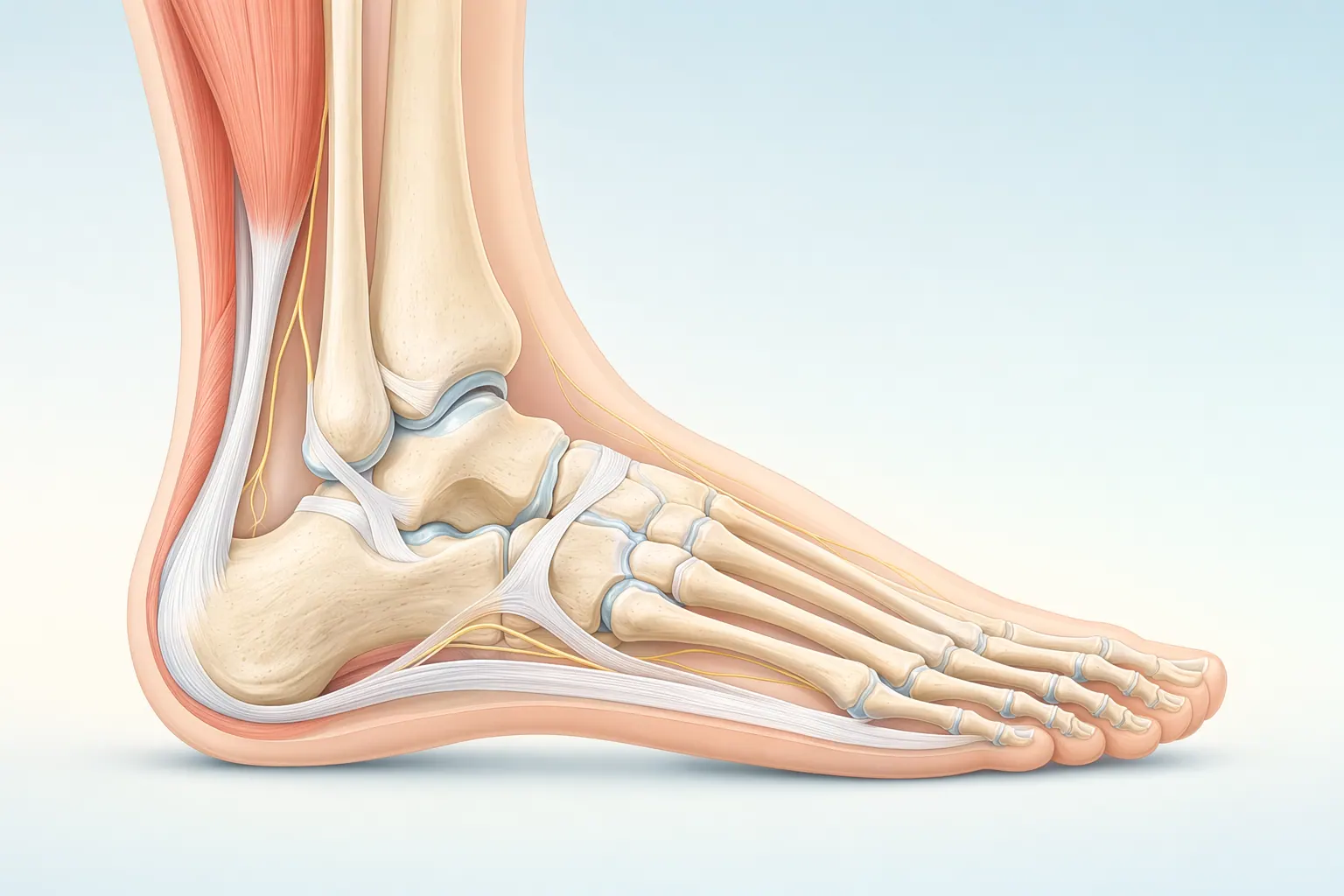
The foot and ankle have 26 bones, more than 30 joints, and over 100 ligaments and tendons. The plantar fascia spans the bottom of the foot, the Achilles tendon anchors the calf to the heel, and the ankle is a hinge that handles every step you take. Most foot and ankle problems trace back to overload, alignment, or footwear that doesn’t match the way your foot is built.
Cheilectomy is an outpatient procedure, usually done under regional or general anesthesia with an ankle or foot block for comfort afterward. Here is what typically happens:
If an exam under anesthesia shows the arthritis is more advanced than expected, your surgeon will have already discussed a backup plan with you (such as adding a small wedge osteotomy of the toe bone, or, for end-stage joints, fusion). You consent to that contingency before surgery, so there are no surprises.
Foot & Ankle care is highly technique-dependent. Volume, training, and judgment together determine the outcome you actually feel six months later.
Our foot & ankle specialists move stepwise — start with the least-invasive option that fits your situation, escalate only when it doesn't.
If most of these match your situation, an evaluation with a foot & ankle specialist is the next step.
These signs typically point toward an in-person evaluation with a foot & ankle specialist.
Your first visit is built to give you an answer the same day, not just another referral.
Recovery is rarely a straight line — but a clear plan with measurable milestones makes the path predictable.
In the first two weeks we focus on protecting the foot & ankle, calming inflammation, and restoring basic motion.
Targeted physical therapy rebuilds strength, mobility, and confidence in the foot & ankle.
Once function is restored, the focus shifts to keeping you there — and catching any recurrence early.
We talk through the risks and benefits with every patient — informed consent is a conversation, not a form.
Every orthopedic intervention carries a small set of standard risks. We screen, prepare, and monitor for these on every patient.
Some risks are tied to the structures we're treating in the foot & ankle. We discuss these in detail at your visit so you can weigh them against the benefits.
At LAOSS, our foot & ankle specialists combine advanced surgical expertise with a patient-first approach. From minimally invasive arthroscopic techniques to reconstruction, fracture care, and arthritis management, our physicians bring decades of experience to every case. Trusted across Los Angeles, our team is dedicated to restoring mobility, relieving pain, and helping you return to the activities you love.
At LAOSS, we treat hallux rigidus conservative-first. Before any surgery is on the table, our foot and ankle specialists try the non-surgical options that often control the pain: stiff-soled or rocker-bottom shoes, a Morton's-extension orthotic or turf-toe plate to limit how far the big toe bends, anti-inflammatory medication, activity modification, and a targeted cortisone injection into the joint. Many patients get real relief from these alone.
When the pain keeps limiting your walking, work, or sport despite conservative care, cheilectomy is often the next logical step for mild-to-moderate arthritis — because it relieves the impingement while preserving the joint you were born with. We will look at your X-rays with you, explain exactly where your arthritis falls on the spectrum, and tell you honestly whether a motion-sparing cheilectomy or a more definitive fusion is the better long-term fit for your joint.
With eight Los Angeles–area offices, on-site imaging at most locations, and fellowship-trained and experienced foot and ankle specialists who perform these procedures themselves, you get a clear diagnosis and a written plan — usually at your first visit, not after a chain of referrals.
Book a visit with a foot & ankle specialist at any of our eight Los Angeles–area offices.




