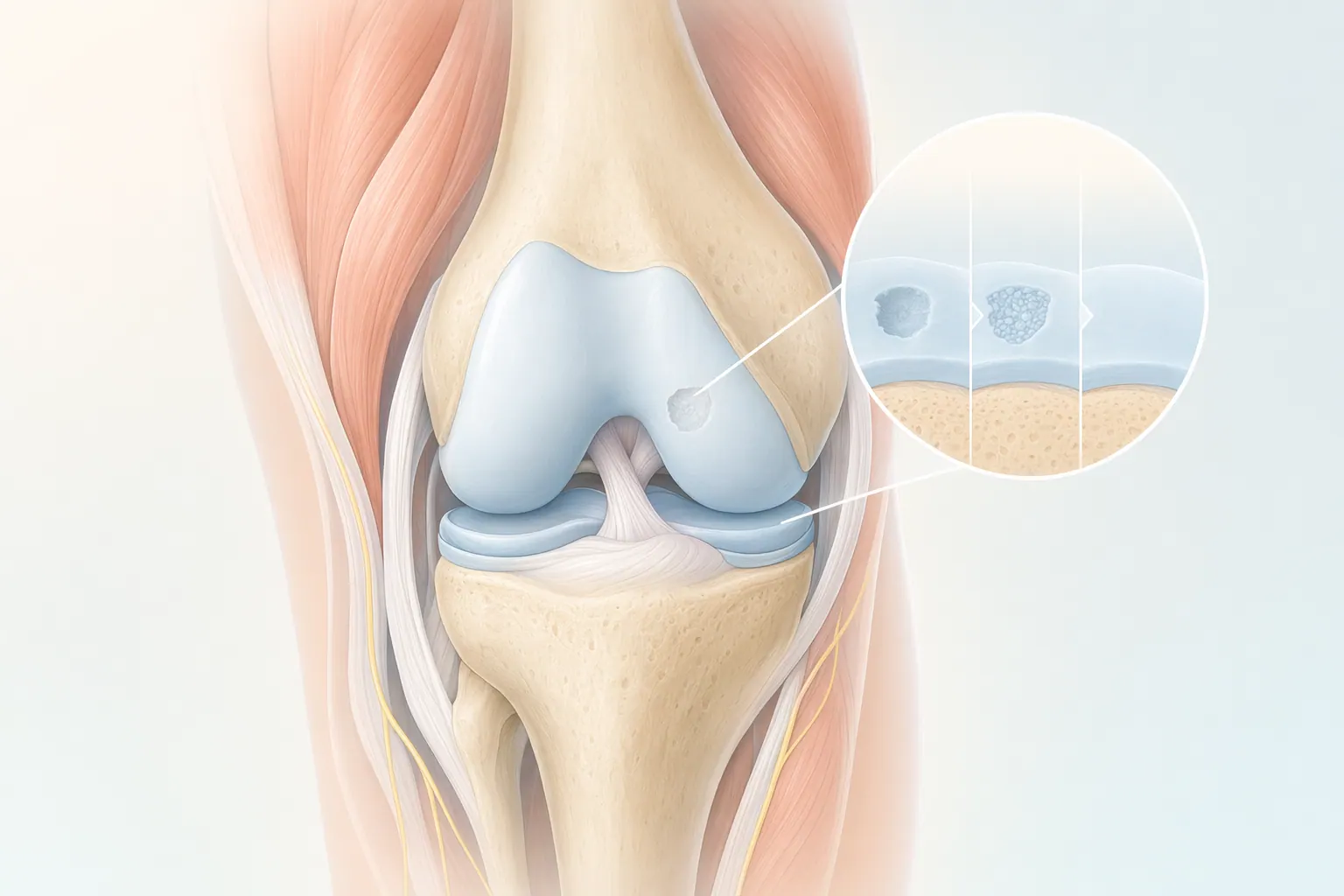
Cartilage reconstruction is a category of joint-preserving surgery that rebuilds damaged cartilage instead of replacing the whole joint. When the smooth articular surface inside a joint is lost — from a sports injury, a fall, osteochondritis dissecans (OCD), or an early-stage focal arthritis lesion — LAOSS surgeons can often restore that surface and keep your own joint working.
The four techniques we use most are microfracture (drilling tiny holes to recruit healing cells), MACI (Matrix-Induced Autologous Chondrocyte Implantation — your own cartilage cells grown in a lab and re-implanted), OATS (Osteochondral Autograft Transfer — moving a small plug of healthy cartilage-and-bone from a non-weight-bearing area), and osteochondral allograft (a matched donor graft for larger defects). Most are performed in the knee, but the same principles apply to the ankle, shoulder, and hip.
This is a different conversation than knee replacement. Cartilage reconstruction is for focal damage in a joint that's otherwise healthy — typically active patients in their 20s, 30s, and 40s who want to stay running, hiking, lifting, or playing for another two or three decades before a replacement is ever on the table.