Common foot & ankle concerns we treat
- Pain that limits walking, standing, or sleep
- Stiffness, swelling, or reduced range of motion
- Sports injuries — acute or overuse
- Arthritis or post-traumatic joint changes
- Conditions other doctors couldn’t resolve
Ankle fusion, or arthrodesis, joins the worn-out ankle bones into one solid unit to eliminate the painful, bone-on-bone motion of end-stage arthritis. LAOSS foot & ankle specialists perform this procedure across eight Los Angeles–area offices, with on-site imaging and conservative-first care before any surgery is considered.

Surgical and non-surgical options at LAOSS.
Ankle fusion (arthrodesis) is the long-standing surgical treatment for end-stage ankle arthritis — the point where the cartilage in the tibiotalar (ankle) joint has worn down to bone-on-bone and pain limits walking, work, and sleep. Instead of replacing the joint, fusion permanently joins the bottom of the shinbone (tibia) to the talus below it, so the two bones grow together into one solid piece. Once the joint no longer moves, the grinding pain of arthritis goes away.\n\nThe most common reason for ankle fusion is post-traumatic arthritis — arthritis that develops years after a serious ankle fracture, repeated sprains, or a pilon or talus injury. It is also used for primary osteoarthritis, inflammatory arthritis such as rheumatoid arthritis, failed previous surgery, and deformity or instability that has destroyed the joint.\n\nThe honest trade-off is motion. A fused ankle no longer bends up and down on its own, so the rocking, rolling part of your step is handled by the neighboring joints in the hindfoot and midfoot. Most people walk well, return to many activities, and are simply grateful to be out of pain — but fusion is a permanent decision, which is why we only recommend it after conservative care has been fully explored and we have discussed how it compares to total ankle replacement.
This surgical procedure is performed to treat severe arthritis or injury of the ankle joint. During the procedure, the surgeon removes damaged bone and cartilage and fuses the joint. This stabilizes the ankle and relieves pain.
Animations licensed from ViewMedica · Swarm Interactive
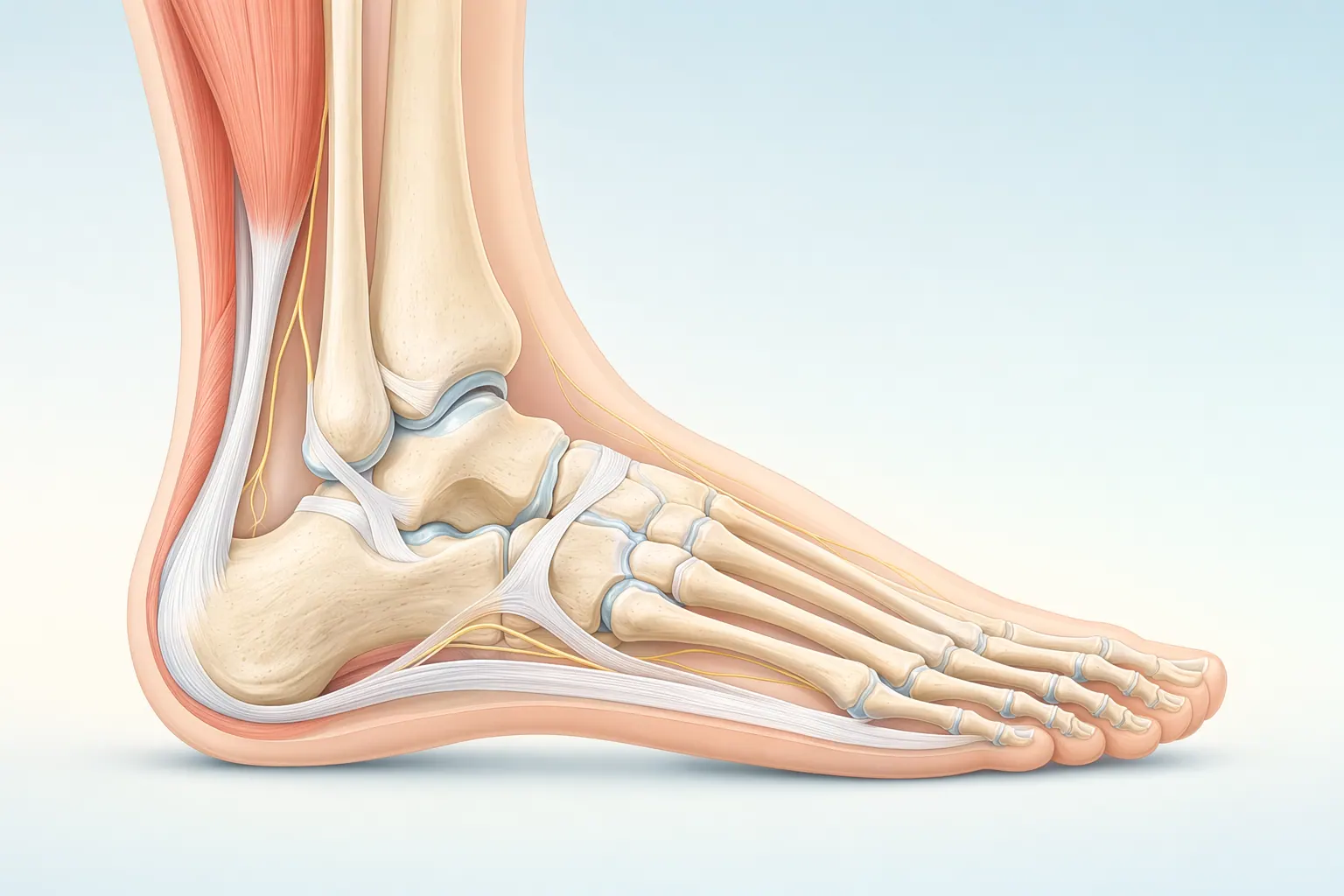
The foot and ankle have 26 bones, more than 30 joints, and over 100 ligaments and tendons. The plantar fascia spans the bottom of the foot, the Achilles tendon anchors the calf to the heel, and the ankle is a hinge that handles every step you take. Most foot and ankle problems trace back to overload, alignment, or footwear that doesn’t match the way your foot is built.
Ankle fusion is done in the operating room under anesthesia, often with a nerve block for post-op comfort. The approach is tailored to your anatomy and the severity of the arthritis.\n\n- Reaching the joint — Your surgeon accesses the ankle either through an open incision or, in select cases, with an arthroscopic (camera-assisted) technique through small portals when alignment is good and the deformity is minimal.\n- Preparing the surfaces — The remaining damaged cartilage is removed from the bottom of the tibia and the top of the talus, exposing healthy bleeding bone. This is the step that allows the two bones to knit together.\n- Setting the position — The ankle is positioned in a neutral, plantigrade alignment (foot flat, slight outward rotation) so you can walk evenly once healed. Getting this position right is critical to a good outcome.\n- Holding it together — The bones are compressed and fixed with hardware — typically screws, a plate, or both, and occasionally an external frame. Bone graft (your own bone or a graft substitute) may be added to encourage fusion, especially when there are gaps or a history of poor healing.\n- Closing and protecting — The incisions are closed and the leg is placed in a splint or cast. You go home the same day or after a short stay, and the cast keeps the ankle still while the bones fuse.
Foot & Ankle care is highly technique-dependent. Volume, training, and judgment together determine the outcome you actually feel six months later.
Our foot & ankle specialists move stepwise — start with the least-invasive option that fits your situation, escalate only when it doesn't.
If most of these match your situation, an evaluation with a foot & ankle specialist is the next step.
These signs typically point toward an in-person evaluation with a foot & ankle specialist.
Your first visit is built to give you an answer the same day, not just another referral.
Recovery is rarely a straight line — but a clear plan with measurable milestones makes the path predictable.
In the first two weeks we focus on protecting the foot & ankle, calming inflammation, and restoring basic motion.
Targeted physical therapy rebuilds strength, mobility, and confidence in the foot & ankle.
Once function is restored, the focus shifts to keeping you there — and catching any recurrence early.
We talk through the risks and benefits with every patient — informed consent is a conversation, not a form.
Every orthopedic intervention carries a small set of standard risks. We screen, prepare, and monitor for these on every patient.
Some risks are tied to the structures we're treating in the foot & ankle. We discuss these in detail at your visit so you can weigh them against the benefits.
At LAOSS, our foot & ankle specialists combine advanced surgical expertise with a patient-first approach. From minimally invasive arthroscopic techniques to reconstruction, fracture care, and arthritis management, our physicians bring decades of experience to every case. Trusted across Los Angeles, our team is dedicated to restoring mobility, relieving pain, and helping you return to the activities you love.
Recovery from ankle fusion is a marathon, not a sprint — the goal is solid bony union, and that takes time and patience.\n\nThe first weeks are spent off the foot. Most patients are non-weightbearing in a cast or boot for roughly 6 to 12 weeks, using crutches, a knee scooter, or a walker, with the leg elevated to control swelling. Your surgeon uses X-rays (and sometimes a CT scan) to confirm the bones are actually fusing before clearing you to bear weight.\n\nAs fusion is confirmed, you transition into a walking boot and gradually build up weightbearing, then move into supportive shoes. Physical therapy focuses on gait, calf and hip strength, and balance — not on bending the fused ankle, which is intentionally rigid. Many people walk comfortably for everyday distances within a few months, with continued improvement over six months to a year as you adjust to the new mechanics.\n\nSmoking, diabetes, and poor circulation meaningfully raise the risk of the bones failing to fuse (nonunion). We screen for these factors ahead of time, and stopping smoking before and after surgery is one of the most important things you can do for a successful result. Over the long term, the neighboring hindfoot and midfoot joints take on more work and can develop arthritis years down the road — a trade-off we explain clearly so the decision is fully informed.
Book a visit with a foot & ankle specialist at any of our eight Los Angeles–area offices.




