Common foot & ankle concerns we treat
- Pain that limits walking, standing, or sleep
- Stiffness, swelling, or reduced range of motion
- Sports injuries — acute or overuse
- Arthritis or post-traumatic joint changes
- Conditions other doctors couldn’t resolve
Flatfoot reconstruction rebuilds a collapsed arch by realigning the heel bone, restoring the failed tendons and ligaments that hold the arch up, and balancing the foot so you can stand and walk without the inner-ankle pain that comes from a fallen arch. At LAOSS, fellowship-trained foot and ankle surgeons across eight Los Angeles-area offices recommend it only after well-run conservative care has been given a fair trial.

Surgical and non-surgical options at LAOSS.
Flatfoot reconstruction is a group of surgical techniques used to correct a collapsed arch that has become painful, deformed, or progressive despite non-surgical care. In adults, the most common reason is adult-acquired flatfoot deformity — usually driven by failure of the posterior tibial tendon, the main tendon that supports and lifts the arch on the inside of the ankle. As that tendon stretches and weakens, the arch flattens, the heel drifts outward, and the front of the foot rotates away from the midline. Over time the soft tissues that backed up the tendon — especially the spring ligament — give way too, and the deformity worsens.
The goal of surgery is not simply to flatten-out a painless arch. It is to relieve pain, re-stack the bones into a more normal alignment, and stop a flexible deformity from progressing into a stiff, arthritic one. A flexible flatfoot — one that still corrects when the surgeon moves it by hand — can usually be rebuilt while preserving the joints. A rigid flatfoot, or one with established arthritis in the hindfoot joints, generally needs a fusion of one or more joints rather than a joint-sparing reconstruction.
Reconstruction is almost always elective and conservative-first. Many people do well for years with custom orthotics, an arch-supporting brace or AFO, a calf-stretching and posterior-tibial strengthening program, anti-inflammatory measures, and activity changes. Surgery is considered when a well-run trial of that care fails to control pain or when imaging shows the deformity is steadily getting worse.
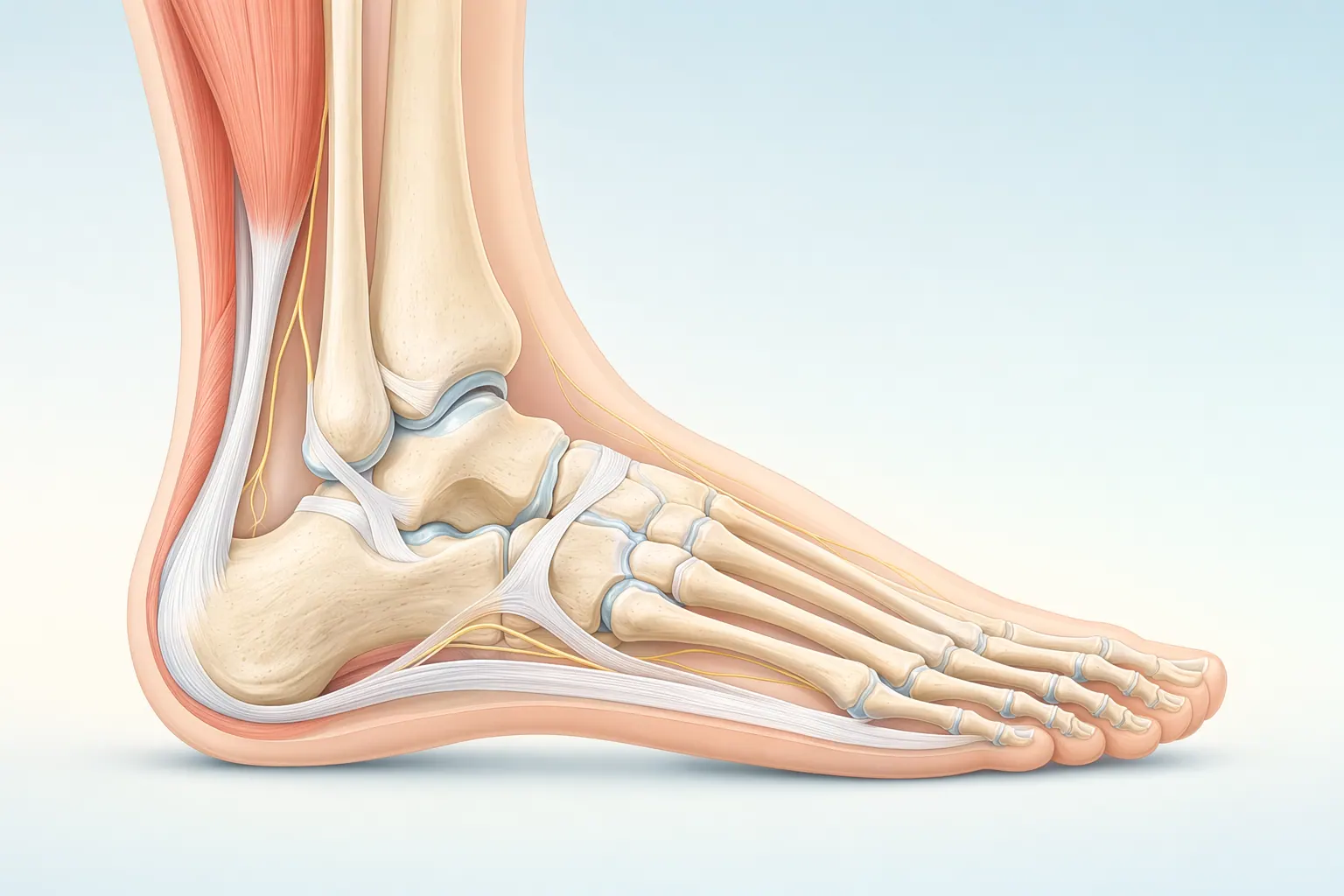
The foot and ankle have 26 bones, more than 30 joints, and over 100 ligaments and tendons. The plantar fascia spans the bottom of the foot, the Achilles tendon anchors the calf to the heel, and the ankle is a hinge that handles every step you take. Most foot and ankle problems trace back to overload, alignment, or footwear that doesn’t match the way your foot is built.
Flatfoot reconstruction is tailored to your specific deformity, so the exact combination of steps differs from patient to patient. For a flexible adult-acquired flatfoot, the surgery usually pairs a bone realignment (osteotomy) with a soft-tissue repair, performed under regional or general anesthesia as an outpatient or short-stay procedure. Common building blocks include:
When the deformity is rigid or arthritic, the plan shifts from rebuilding to fusing the affected hindfoot joints — a double or triple arthrodesis — which corrects the alignment and reliably relieves pain but trades some motion for stability. Your surgeon decides between these paths using your exam and weightbearing imaging, and walks you through the specific combination before the day of surgery.
Foot & Ankle care is highly technique-dependent. Volume, training, and judgment together determine the outcome you actually feel six months later.
Our foot & ankle specialists move stepwise — start with the least-invasive option that fits your situation, escalate only when it doesn't.
If most of these match your situation, an evaluation with a foot & ankle specialist is the next step.
These signs typically point toward an in-person evaluation with a foot & ankle specialist.
Your first visit is built to give you an answer the same day, not just another referral.
Recovery is rarely a straight line — but a clear plan with measurable milestones makes the path predictable.
In the first two weeks we focus on protecting the foot & ankle, calming inflammation, and restoring basic motion.
Targeted physical therapy rebuilds strength, mobility, and confidence in the foot & ankle.
Once function is restored, the focus shifts to keeping you there — and catching any recurrence early.
We talk through the risks and benefits with every patient — informed consent is a conversation, not a form.
Every orthopedic intervention carries a small set of standard risks. We screen, prepare, and monitor for these on every patient.
Some risks are tied to the structures we're treating in the foot & ankle. We discuss these in detail at your visit so you can weigh them against the benefits.
At LAOSS, our foot & ankle specialists combine advanced surgical expertise with a patient-first approach. From minimally invasive arthroscopic techniques to reconstruction, fracture care, and arthritis management, our physicians bring decades of experience to every case. Trusted across Los Angeles, our team is dedicated to restoring mobility, relieving pain, and helping you return to the activities you love.
Flatfoot reconstruction is a real recovery, not a quick procedure, because cut bone has to heal in its new position before it can bear weight. Most patients spend roughly the first six weeks non-weightbearing in a cast or splint, then transition to a walking boot as the osteotomies knit. Crutches, a knee scooter, or a walker get you around safely during that protected period, and elevation in the early days is important for swelling and wound healing.
Around the 6-to-12-week mark, as X-rays confirm bone healing, you gradually progress to full weight in the boot and begin physical therapy to rebuild ankle and foot motion, calf and posterior-tibial strength, and balance. Many patients move into a supportive shoe with an orthotic over the following weeks. Swelling is common for months and tends to be worse at the end of the day — that is expected and improves slowly.
Return to low-impact activity is often in the range of a few months, while higher-impact activity and sport typically take longer, frequently into the six-month-plus range depending on which procedures were done and how the bone heals. Desk work can sometimes resume within a few weeks with the leg elevated; jobs that require standing, walking, or labor take considerably longer. Your specific timeline depends on the combination of osteotomy, tendon transfer, and any fusion performed, and your LAOSS surgeon will give you milestones specific to your case.
Like any reconstruction, it carries surgical risks worth discussing in advance — including infection, delayed or incomplete bone healing (nonunion), nerve irritation or numbness along the foot, hardware that occasionally needs removal, blood clots, residual or recurrent deformity, and stiffness. These are uncommon, and we screen and plan for them, but informed consent is a conversation we have with every patient.
Book a visit with a foot & ankle specialist at any of our eight Los Angeles–area offices.




