What patients ask us most
- Will I get my overhead reach back?
- Why does my surgeon want a reverse instead of an anatomic?
- Is one more durable than the other?
- What's the real difference in recovery?
- Can I go back to golf, swimming, or yoga?
If you're weighing a reverse total shoulder (rTSA) against an anatomic total shoulder (aTSA), the answer almost always comes down to one thing — your rotator cuff. Both procedures are excellent at relieving pain. They are not interchangeable. Our LAOSS shoulder surgeons walk you through what each operation actually does, who it fits, and why the decision is anatomy-driven, not preference-driven.

Same goal — pain relief. Two very different operations.
Both procedures treat a worn-out, painful shoulder and both can be life-changing. But they solve different mechanical problems, and the choice between them is almost entirely driven by the state of your rotator cuff.
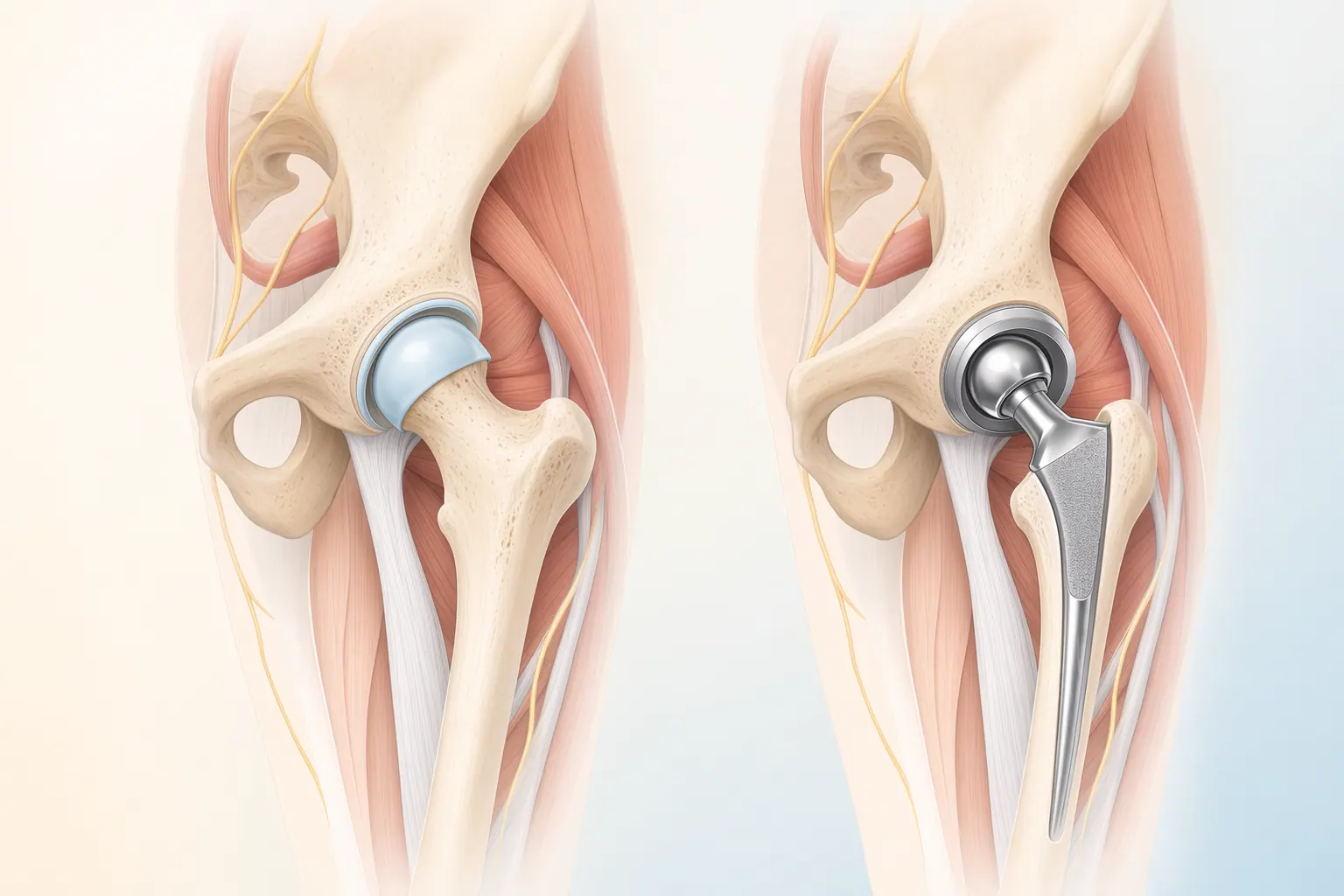
Anatomic total shoulder arthroplasty (aTSA) mirrors the shoulder you were born with. The arthritic humeral head is replaced with a metal ball and the worn glenoid socket is resurfaced with a polyethylene cup. The rotator cuff still does the work of lifting and rotating your arm, just now over smooth artificial surfaces. It's the procedure of choice for primary glenohumeral osteoarthritis in a patient with an intact, functional rotator cuff — typically a younger or middle-aged adult who wants the most natural-feeling shoulder possible.
Reverse total shoulder arthroplasty (rTSA) flips the geometry. A metal ball is anchored to the glenoid (the socket side) and a polyethylene cup is placed on the humerus (the arm side). That reversal lets your deltoid muscle — the big triangular shoulder muscle — take over the job of lifting your arm overhead. It's the answer when the rotator cuff can't reliably do that work anymore: massive irreparable cuff tears, rotator cuff arthropathy, complex proximal humerus fractures in older adults, and salvage of failed prior shoulder surgery.
The most important point: both procedures are excellent at pain relief. Where they differ is mechanics. Reverse is the only durable option when the cuff is gone, even though anatomic tends to give slightly better forward elevation in patients whose cuff is intact. The decision-driver is anatomy, not preference.
This surgery replaces the damaged surfaces of your shoulder joint with implants that move like a healthy shoulder. It can relieve pain and restore meaningful motion.
Animations licensed from ViewMedica · Swarm Interactive
The shoulder is a ball-and-socket joint, but it's a shallow socket held in place by the rotator cuff — four small muscles that center the humeral head and provide the leverage you need to lift your arm. An anatomic replacement recreates that native geometry and relies on the rotator cuff to keep working. A reverse replacement intentionally moves the center of rotation and lengthens the deltoid's lever arm so it can lift the arm on its own — no rotator cuff required. That single design change is why reverse shoulder works in patients where anatomic shoulder would fail.
Choosing between an anatomic and a reverse shoulder isn't a personality match — it's a structured set of questions our shoulder surgeons answer at your evaluation.
The exam: How much active motion do you actually have versus passive motion? A shoulder that you can't lift but that the surgeon can lift for you points toward cuff weakness and that pushes us toward reverse. We test the strength of each rotator cuff muscle individually, look for lag signs, and assess the deltoid carefully (the deltoid has to be working for a reverse to succeed).
Imaging: Weight-bearing X-rays show joint space, glenoid wear pattern, and whether the humeral head has migrated upward — a classic sign of long-standing cuff tear and a strong indicator toward reverse. An MRI or ultrasound of the rotator cuff is essential. We're asking specific questions: Is the cuff intact? If torn, is it repairable, or is the tendon retracted and the muscle fatty-infiltrated? A CT scan is often added to assess glenoid bone stock, especially in revisions or in patients with significant posterior wear.
Patient profile: Age, activity goals, hand dominance, and the demands you place on the shoulder all factor in. A 58-year-old golfer with primary OA and a healthy cuff is a textbook anatomic candidate. A 75-year-old with cuff arthropathy and pseudoparalysis is a textbook reverse candidate. Plenty of patients sit in the middle, and that's where careful imaging review matters most.
Most LAOSS patients leave their first evaluation with the imaging in hand, a clear diagnosis, and a written plan that names a specific procedure and explains why.
Both paths start from the same conservative-care foundation — activity modification, PT, injections, and time. Where they diverge is the surgical decision, and that decision is almost entirely about the rotator cuff and the shape of your glenoid.
The right call when the rotator cuff is intact and the arthritis is the dominant problem. Anatomic tends to give the most natural-feeling shoulder when the biology supports it.
The right call when the rotator cuff cannot reliably do its job. Reverse is more forgiving of complex anatomy and is often the only durable option in these scenarios.
The biggest difference between the two procedures isn't the materials — it's the geometry. That geometry decides which muscle does the lifting and which patients can rely on it.
Anatomic shoulder restores the joint surfaces and lets your existing muscles work the way they always have. The rotator cuff centers the humeral head; the deltoid powers the lift. When the cuff is healthy, the result is a remarkably natural-feeling shoulder.
Reverse shoulder moves the ball to the scapula and the cup to the humerus. That shift lengthens the deltoid's lever arm and lets it lift the arm overhead without help from the rotator cuff. It's a fundamentally different machine designed for a fundamentally different problem.
Day-to-day recovery is similar — both procedures live in a 3 to 6 month rehab window. Where they differ is the motion ceiling at the end of rehab, especially overhead and behind-the-back reach.
Most LAOSS anatomic shoulder patients spend a night in the hospital, wear a sling for about 4 to 6 weeks, and start a structured PT program early. Most are back to driving and desk work within 2 to 6 weeks.
Early recovery looks similar — a sling, early gentle motion, and a structured PT program. Reverse is often faster to feel comfortable in the first weeks because the new geometry takes pressure off the cuff completely.
Both implants are designed to last decades. Registry data and patient profile drive different real-world failure patterns.
Modern anatomic shoulder implants show excellent survivorship in the right patient — typically 90% or better at 10 to 15 years when the rotator cuff stays healthy.
Reverse shoulder survivorship has improved markedly with modern designs. Most series show survivorship comparable to anatomic at 10 years, with continued data accumulating beyond that.
Shoulder replacements of both kinds are revisable, but the strategies differ. Catching the problem early is the common theme — which is why your LAOSS surgeon will keep you on a follow-up schedule even when you feel completely fine.
Shoulder arthroplasty is one of the most volume-sensitive procedures in orthopedics. Surgeon volume predicts outcome more reliably than implant brand, and component positioning is unforgiving — especially on the glenoid side of a reverse.
We do both procedures and we choose between them based on the rotator cuff, the glenoid, and the patient in front of us, not on which operation is trending. Most patients leave the first visit with a specific recommendation and the reasoning behind it.
If most of the items in either column match your situation, an evaluation with a shoulder specialist is the next step. Many patients fit one column cleanly and that's usually the right answer.
Anatomic shoulder is for the patient whose biology can still drive a natural-feeling shoulder.
Reverse shoulder is for the patient whose cuff cannot reliably power the arm anymore or whose anatomy needs a more forgiving design.
Whether you have an anatomic or a reverse shoulder, the first 6 weeks look similar. The differences show up in the 3 to 6 month window as we clear specific motions and loads.
Most patients spend a night in the hospital and go home with their arm in a sling. The first two weeks focus on pain control, wound healing, and protected motion.
Structured PT rebuilds motion, strength, and confidence. The early phase is passive; active strengthening begins after the sling comes off.
Once basic function is restored, the focus shifts to long-term activity goals and that's where anatomic and reverse paths diverge in subtle ways.
Both procedures carry the same baseline surgical risks plus a smaller set of risks specific to the implant design. We talk through all of these at your evaluation — informed consent is a conversation, not a form.
Every shoulder arthroplasty carries the same baseline risks. We screen, prepare, and monitor for these on every patient.
Each design carries a small set of risks tied to its mechanics. None of these should change the decision when the indication is clear, but they're worth understanding.
Dr. Hayk Stepanyan, Dr. Jayson Lian, Dr. Leah Cyran, and Dr. Sevag Bastian make up the LAOSS shoulder and sports team. Between them they cover the full range of shoulder care from cuff repair and labral surgery to anatomic and reverse total shoulder arthroplasty.
We don't pick anatomic because it's traditional, and we don't pick reverse because it's the newer tool. We look at the cuff, the glenoid, the deltoid, the bone stock, and the patient in front of us and we explain the reasoning out loud. Most patients leave their first LAOSS visit with a specific recommendation, the imaging review that supports it, and an honest answer to the question almost every patient asks: 'will I get my shoulder back?'
Dr. Stepanyan walked me through why a reverse made more sense than the standard replacement because of my cuff tear. Six months later I can reach the top cabinet again and I sleep through the night.
Book a visit with a LAOSS shoulder surgeon at any of our eight Los Angeles area offices. Bring your imaging if you have it — we'll tell you which procedure actually fits your shoulder, and why.




